Ian Byram, MD
Read complete study: Comparison of patient-specific instruments with standard surgical instruments in determining glenoid component position: a randomized prospective clinical trial
The authors of this randomized clinical study compared 15 anatomic total shoulder arthroplasties performed with patient-specific instrumentation to 16 aTSA cases performed with standard surgical instrumentation. Preoperative three-dimensional CT scan images were utilized in both groups to plan the desired implant position, then postoperative CT scans were performed to measure the differences between the intended and actual glenoid implant position. The authors reported improved accuracy of the PSI group with statistically significant decreases in mean deviation of inclination and medial-lateral offset as compared to the standard group. Mean deviation in version was 4.3° ± 4.5° for the PSI group as compared to 6.9° ± 4.4° in the standard surgical group (p=0.11), with significant improvement in version accuracy in patients with preoperative retroversion in excess of 16°. The authors conclude that surgical accuracy is improved by patient specific instrumentation when compared to standard surgical instrumentation, with greatest benefit occurring in patients with severe glenoid deformity.
As technology continues to progress, we will have increased opportunities to improve surgical accuracy in shoulder arthroplasty implant positioning. These are exciting times, but it is our duty to balance cost and utility with progress. The current study brings up several interesting points that impact my practice:
- Preoperative planning with three-dimensional imaging has greatly improved our knowledge and performance in glenoid implant positioning
- Intraoperative instrumentation and/or guidance does improve accuracy
- The desired correction of retroversion remains undetermined
By preoperatively templating, I can more reliably enact a surgical plan to meet the needs of my patients, and this should be considered standard of care in shoulder arthroplasty.
Regarding preoperative planning, I routinely obtain preoperative CT scans with three dimensional reconstructions on nearly all shoulder arthroplasty candidates. The arthritic glenoid does not wear in two dimensions but often with subtle variations that may not be obvious on axillary radiographs or even axial CT cuts alone. By preoperatively templating, I can more reliably enact a surgical plan to meet the needs of my patients, and this should be considered standard of care in shoulder arthroplasty. In patients with a central wear pattern that have already obtained an MRI to assess the integrity of the rotator cuff I will consider planning based on this study alone, but this is generally only for cost purposes or patient convenience.
With regard to the second point, this study shows how intraoperative guidance can improve accuracy in glenoid positioning, with the greatest benefit seen in patients with severe deformity. It has been shown numerous times that anatomic placement of implants leads to improved clinical outcomes in shoulder arthroplasty. Intraoperative guidance can be in the form of PSI (as seen in this study), custom implants, or computer guided intraoperative navigation. In my practice, I have begun to implement CT guided navigation for glenoid implantation. PSI and computer navigation both offer the ability to improve accuracy, but PSI does not allow for intraoperative corrections such as conversion to reverse arthroplasty or difficulty applying the PSI guide due to anatomical constraints. In this study, 3 of the 44 patients initially enrolled for anatomic TSA underwent reverse TSA, eliminating them as candidates for PSI.
As an example, the following case is a 67 year old male with a retroverted glenoid and intact rotator cuff based on exam and preoperative imaging.
My initial plan was anatomic TSA with partial version correction using an augmented glenoid.
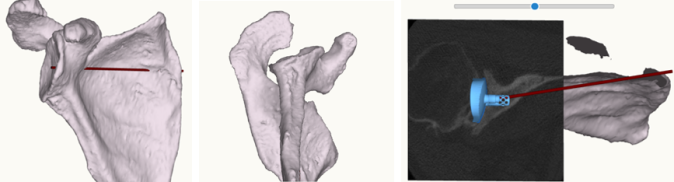
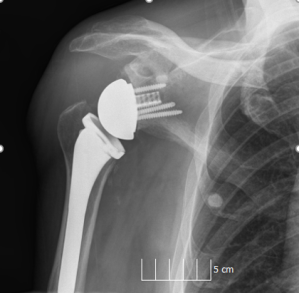
Intraoperatively, the anterosuperior rotator cuff was deficient, with the supraspinatus peeling off the greater tuberosity during humeral dislocation. Using intraoperative computer navigation, I was able to convert to reverse TSA with a posterior augmented baseplate.
Regarding the last point, the authors of this manuscript admit that the “desired” position of the implants in the standard surgical group may be flawed. They attempted to achieve 0° inclination and 0° version, then compared postoperative implant position to these “ideal” goals. In the PSI group, the surgeons attempted to match the patients’ native version and inclination based on the vault model method. As such, there was likely less version correction on average in the PSI group – an easier goal to attain than that of the standard group. Placing a glenoid implant at 0° version is likely not ideal in many cases. Surgeons must rely on factors such as humeral head subluxation, amount of bone reaming required to correct version, and native anatomy to help determine surgical goals. I would caution against attempting to achieve 0° version in every case, as this may lead to over-reaming of the glenoid, medialization of the joint line, and overuse of augmented glenoid implants. Improvements in technology such as PSI and computer navigation are helpful intraoperative tools, but the successful surgery still requires appropriate preoperative planning.
Ian Byram, MD, is a shoulder and elbow specialist at the Bone and Joint Institute of Tennessee. Dr. Byram received his medical degree from the University of North Carolina School of Medicine and completed his residency at Vanderbilt University School of Medicine. He went on to complete a shoulder, elbow and sports medicine fellowship at Columbia University Medical Center. Dr. Bryam is an accomplished author of more than 20 peer-review articles and book chapters, and member of several professional societies.