Kevin Famer, MD
Read complete study: Reverse total shoulder glenoid baseplate stability with superior glenoid bone loss
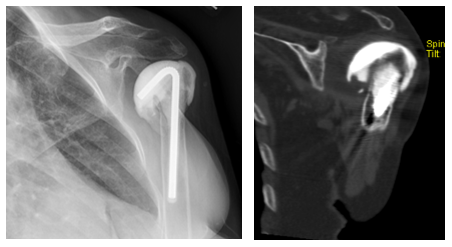
In the article “Reverse total shoulder glenoid baseplate stability with superior glenoid bone loss” by Martin et al, the authors looked to quantify glenoid baseplate stability with worsening superior glenoid bone loss. The authors utilized a polyurethane bone model, and created superior glenoid bone loss defects such that the attached baseplates had 100% support, 90% support, 75% support, and 50% support. The authors found the 50% support group had significantly greater micromotion than the other defects and the native state. The majority of micromotion occurred at the beginning of testing, indicating that some settling may occur with time. Interestingly, micromotion in the 50% support group exceeded 150 µm, which has been shown in animal models to be the maximum amount of micromotion that allows bony ingrowth.
The authors spend a lot of time describing their testing methods, compared to other published manuscripts. The authors applied cyclic loading at a fixed 60º glenohumeral angle, which mimics the superiorly directed force during the initiation of abduction, as opposed to other studies that apply force to the baseplate that mimics the force during the range of abduction. The benefits of the study design of this current study is that it allows real time assessment of micromotion during the course of the analysis, as well as pre and post testing, potentially allowing a better assessment of micromotion early in the loading process.
The information presented in this study is valuable in the sense that using real time of assessment of micromotion, the authors find that increasing superior glenoid wear leads to increasing superior micromotion early in the loading process. There also appears to be some settling over time, but the issue failure of early bony integration, and its association to loosening over time, is a concern. Surgeons should be aware of results of this study, and the potential risk of glenoid loosening with uncorrected superior glenoid wear.
When approaching superior glenoid wear, surgeons have three main options.
The first is eccentric reaming to ream down the high side, in this case, the inferior glenoid. While this corrects the superior inclination of the glenoid and addresses some wear patterns, it does so at the expense of reaming down subchondral bone, and effectively medializing the glenoid. Reaming subchondral bone and medializing the baseplate, although effective in correcting some glenoid deformities, could potentially lead to poor glenoid fixation, instability issues, and increased notching risks. Given these concerns, this technique is limited to minor defects.
The second option available to surgeons is bone grafting of the glenoid. This can performed with autograft, such as the humeral head, or allograft. Good outcomes have been reported using this technique, but there is a risk of poor graft incorporation. Although Jones et al. have reported good outcomes using this technique, they also reported 20% of grafts with failure to incorporate, and 6/44 (14%) baseplates considered loose. Although this technique is a popular option for glenoid deficiencies, the concerns for poor incorporation and subsequent baseplate loosening should be considered.
The final option available to surgeons is an augmented baseplate. Augments for superior wear, posterior wear, and postero-superior wear are available. These options allow surgeons to ream off-axis, which minimizes the amount of subchondral bone removed and medialization of the glenoid. Roche et al. demonstrated similar biomechanical properties of eccentric reaming with a standard baseplate and off-axis reaming with a superior augmented baseplate. In addition, Jones et al. demonstrated decreased complications and notching when comparing bone grafting vs. augmented baseplates for glenoid wear.
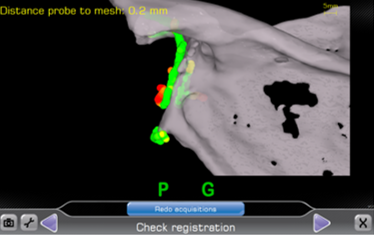
Recently, I have incorporated the use of navigation to assist in proper glenoid placement, making even the most challenging cases more straight forward.
Author’s preferred technique:
Early in my career, my preferred techniques were a combination of eccentric reaming and bone grafting for glenoid defects. Although this worked well, I had a few cases of grafts that resorbed, leaving some baseplates I would term “at-risk”. Over the last five years, I have utilized a 10º superior augment baseplate. This has allowed me to approach these cases with minimal subchondral bone removal, and without having to rely on bone graft incorporation. Recently, I have incorporated the use of navigation to assist in proper glenoid placement, making even the most challenging cases more straight forward. The combination of an augment baseplate and navigation has allowed me to avoid the scenario studied in this paper where the baseplate is at risk for micromotion due to lack of glenoid support.

REFERENCES
Jones RB, Wright TW, Roche CP. Bone Grafting the Glenoid Versus Use of Augmented Glenoid Baseplates with Reverse Shoulder Arthroplasty. Bull Hosp Jt Dis (2013). 2015 Dec;73 Suppl 1:S129-35.
Jones RB, Wright TW, Zuckerman JD. Reverse total shoulder arthroplasty with structural bone grafting of large glenoid defects. J Shoulder Elbow Surg. 2016 Sep;25(9):1425-32.
Roche CP, Stroud NJ, Martin BL, Steiler CA, Flurin PH, Wright TW, Zuckerman JD, Dipaola MJ. Achieving fixation in glenoids with superior wear using reverse shoulder arthroplasty. J Shoulder Elbow Surg. 2013 Dec;22(12):1695-701.
Kevin Farmer, MD, is associate professor in the division of sports medicine at University of Florida and a team physician. Dr. Farmer completed his residency at Johns Hopkins University and fellowships at the Uribe, Hechtman, Zvijac Sports Medicine Institute and the University of Florida.