Moby Parsons, MD
The Ream and Run shoulder replacement is a great option for younger patients with shoulder arthritis who have failed conservative treatment yet wish to maintain a high level of activity. Because the weak link in shoulder replacement is the plastic socket implant, avoiding the insertion of this reduces the risk of failure, particularly for patients who intend to subject their shoulder to moderate stress over a long period of time. The Ream and Run resurfaces the ball, removes the bone spurs, releases the contracted tissues and reshapes the worn socket to a smooth and conforming concavity to mate with the ball.
While partial shoulder replacement (hemiarthroplasty) has historically gotten a bad reputation for having inferior results to total shoulder replacement, the results cannot be generalized to all cases. Many glenoids (socket) have substantial wear and erosion from the arthritic process. If such wear is not addressed at the time of hemiathroplasty, patients are at high risk of continued pain and abnormal joint mechanics. The Walch classification shows the different patterns of wear with the B1, B2 and B3 being both common and problematic. In these patterns, the ball shifts to the back of the arthritic socket and results in progressive erosion of the posterior glenoid. Failure to recenter and reshape the head into a single concavity will result in failure of hemiarthroplasty.

The principle goal of the Ream and Run is to address abnormal socket wear and subluxation of the head allowing the resurfaced head to recenter into a single smooth congruent socket that allows stable rotation with distributed load. Spherical reaming of the socket with preservation of the labrum can accomplish this; however, care must be taken not to over-ream the glenoid as this can expose the soft bone under the joint surface allowing progressive erosion after surgery.
Preoperative planning tools now allow us a detailed 3-D, quantitative assessment of glenoid wear and can be used to plan the optimal corrective reaming that will balance the goals of reshaping the surface and restoring the orientation. Using the ExactechGPS navigation system along with customized glenoid reamers, this plan can then be accurately replicated during the surgery using intelligent instruments that register the plan to the patient’s actual anatomy. This allows real-time, precise glenoid preparation, minimizing the risk of over-reaming.
The following picture demonstrates navigating reaming. The image in the top right image below shows the real-time feedback, showing the surgeon the reamer position and depth relative to the patients glenoid. The use of trackers on the patient’s coracoid process an on the reamer handle allows registration of the patient’s anatomy with the preoperative plan so that the surgeon can execute the plan with a high degree of accuracy. Studies have demonstrated that the ExactechGPS system improves the accuracy of glenoid preparation from + 10 degrees to + 2 degrees.

The following is a case example. This patient is a 70-year-old competitive power lifter with severe bilateral shoulder arthritis. He intends to return to competition and thus will place substantial loads across his shoulder that risk failure of a total shoulder arthroplasty. He has elected to proceed with a Ream and Run.
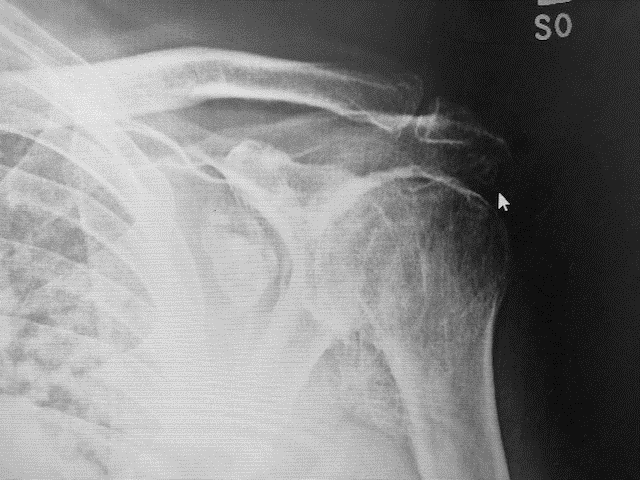

His X-rays show advanced arthritis with large loose bodies and spurs around his glenoid. His CT images confirm large posterior bone spurs.
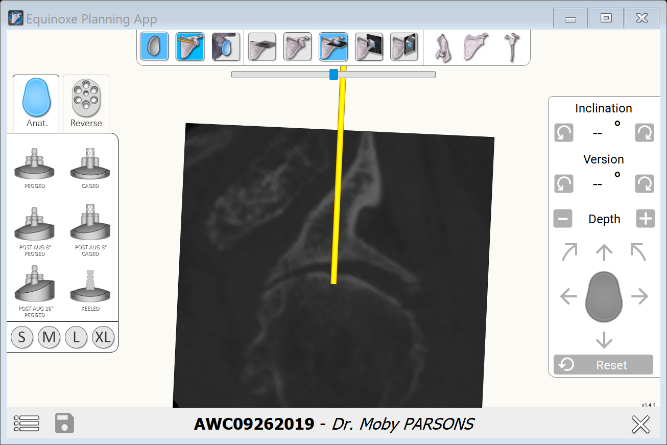
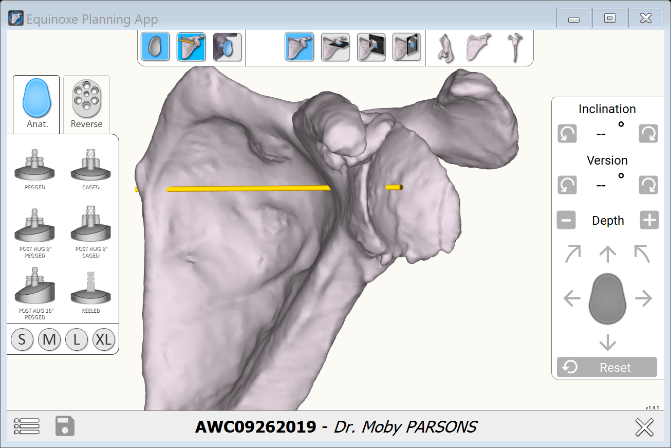
We can plan the Ream and Run by selecting a standard keeled glenoid component. Even though we will not insert this during surgery, we can orient it relative to the glenoid face to model the correction we wish to achieve. In other words, we can plan the case as if we were going to perform a total shoulder using a non-augmented implant. Then, instead of just inserting the implant, the bone is prepared in the same way but using customized reamers with a radius of curvature 2mm greater than the head diameter we select.

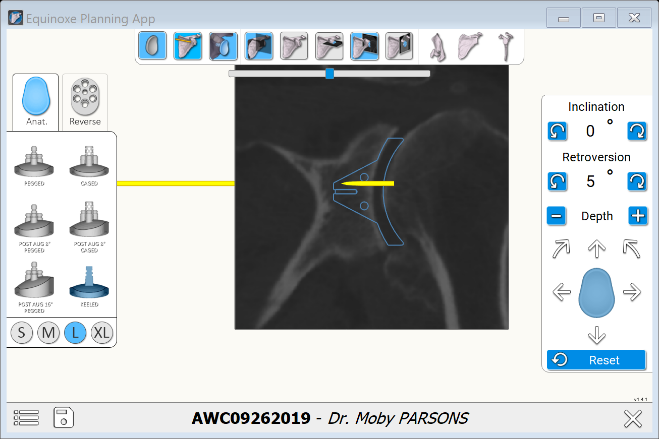
In this case, we can reshape him to 5 degree of retroversion and neutral inclination with minimal corrective reaming. The CT images also show us how much bone spur to remove around the periphery of the socket.
The following are his postoperative images demonstrating a nice congruity of the ball in the reamed socket with a stemless humeral arthroplasty.
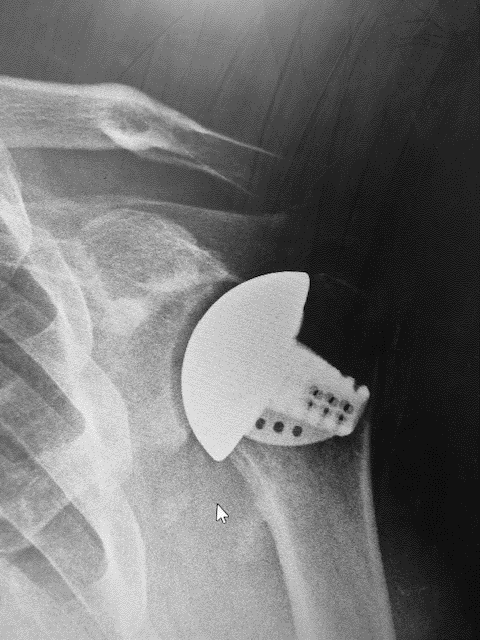
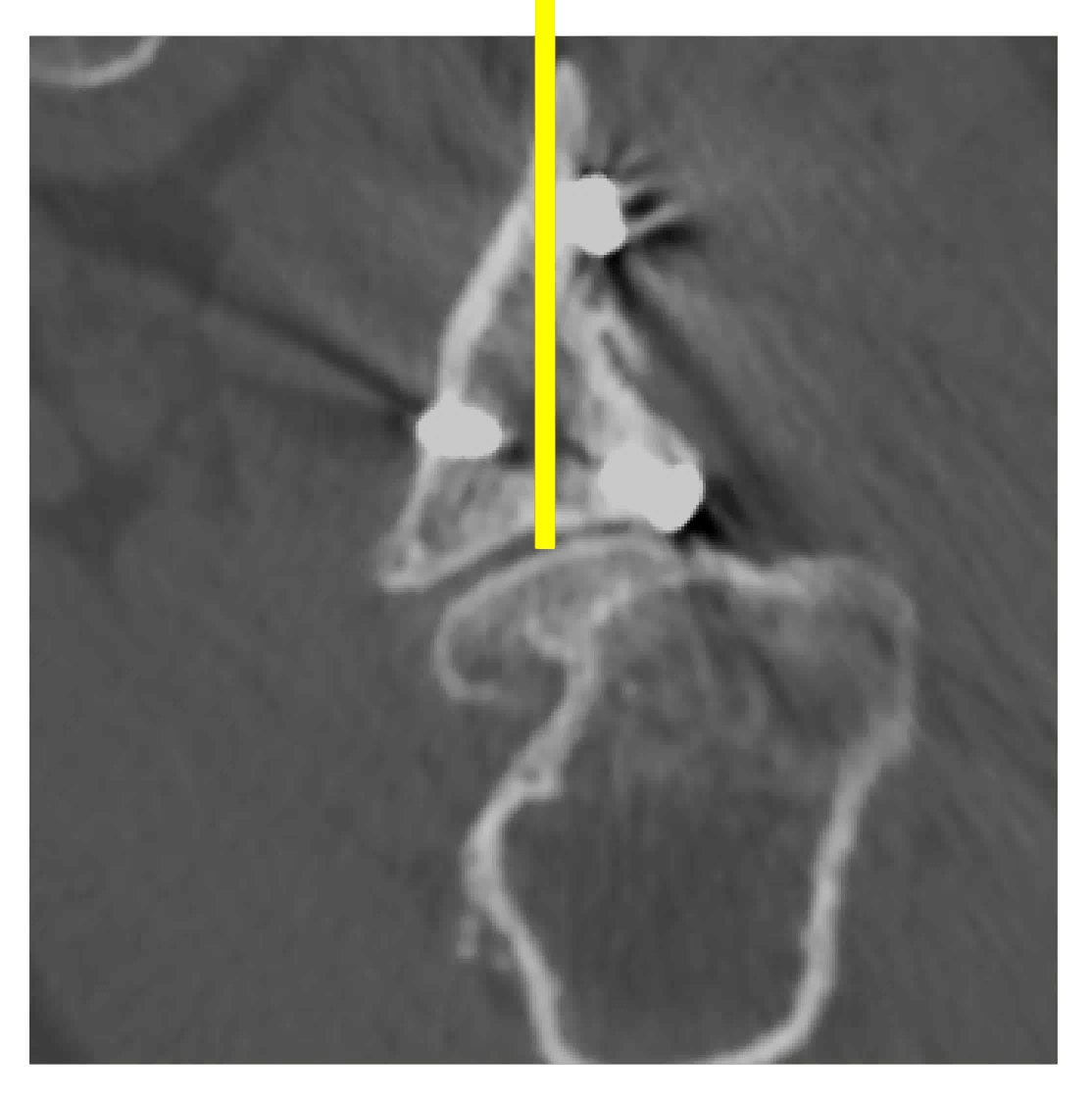
The next case is a 52-year-old motorcycle-racing teacher who previously fractured his scapula and glenoid and has gone on to develop progressive arthrosis and posterior humeral subluxation.


In this case, the preoperative planning can show us that one of the screw heads is protruding into the joint and will need to be removed prior to corrective reaming.

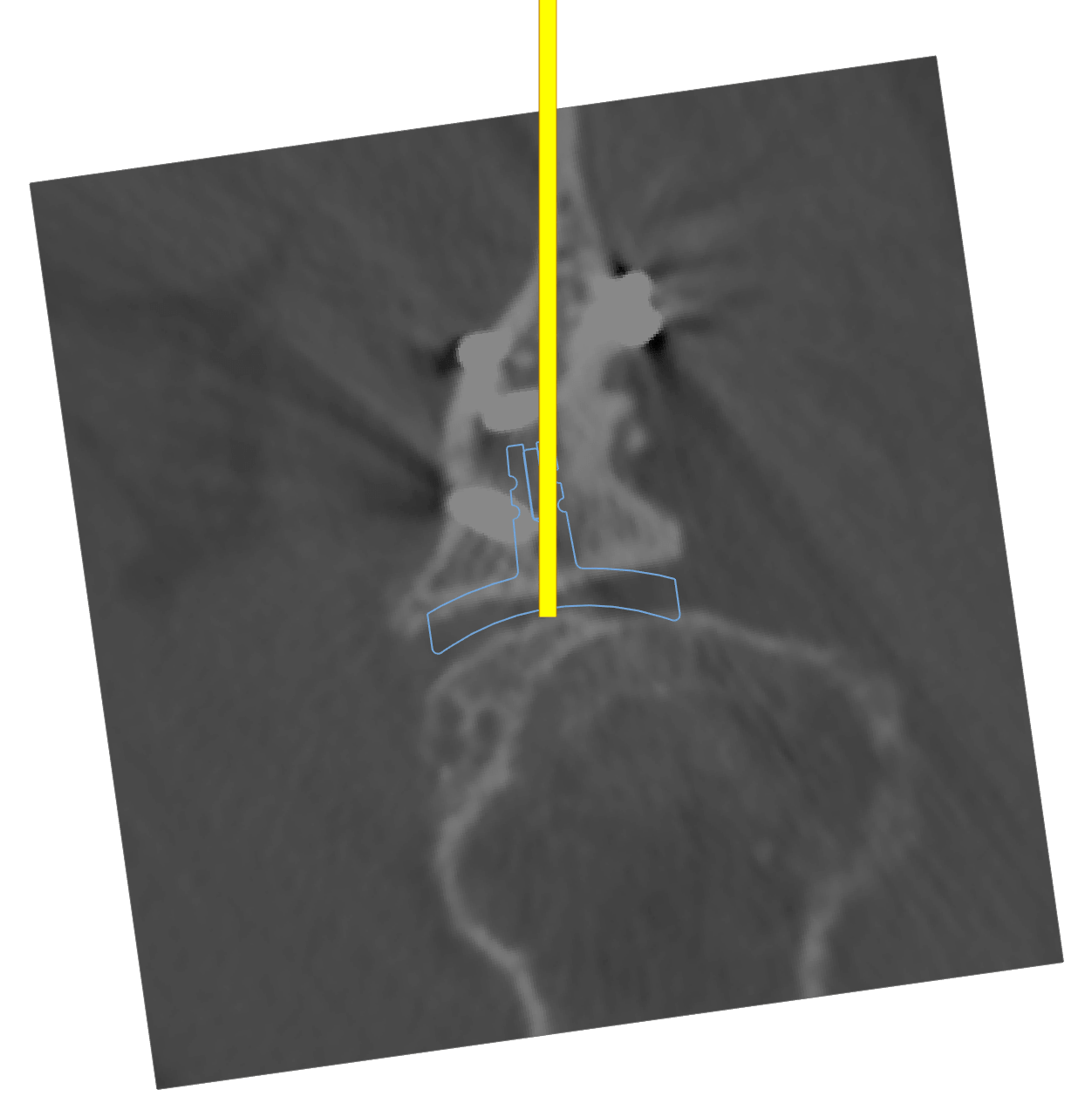
Here we can use the same technique to position a standard glenoid component as a surrogate to plan the corrective reaming. In his case, to avoid removal of excess subchondral bone, we have chosen to leave him in 8 degrees of retroversion relative to the Friedman axis.

His postoperative X-rays show a resurfacing humeral head prosthesis with a nicely recentered humeral head and excellent congruity on the axillary lateral X-rays. He is now back to competitive motorcycle racing and instructing.


Using the ExactechGPS navigation, for the first time, we can quantitatively plan and perform the glenoid preparation in Ream and Run Arthroplasty. This can optimize our reconstruction by balancing the goals of correcting pathologic retroversion, minimizing bone loss through reaming, and creating a smooth concavity. When these goals are combined with proper patient selection and education, excellent surgical technique preserving the labrum and maximizing releases to restore range of motion; and finally, dedicated physical therapy, and durable results comparable to total shoulder arthroplasty can be achieved without the long-term risk of glenoid failure.
Moby Parsons, MD, is in private practice in New Hampshire. He completed his internship and residency at University of Pittsburgh and fellowships at the University of Washington, Southern California Orthopaedic Institute and the University of Sydney. His work has produced multiple published articles and international presentations.