Joseph Zuckerman, MD
Read complete study: A patient Specific guide for Optimizing custom made glenoid implantation in cases of severe glenoid defects.
These authors studied the ability to implant a custom glenoid component in 10 cadaver glenoids with glenoid defects using patient-specific guides and traditional non-guided techniques. The use of the patient-specific guide reduced angular deviations from the plan and significantly improved the position and length of the screw placements when used to implant the custom made glenoid components.
Literature Review:
The authors have focused on a well-known challenge in shoulder arthroplasty – treatment of the deformed glenoid during anatomic or reverse shoulder arthroplasty. There is no doubt that two approaches canbe developed to address this issue. The first is the use of patient-specific guides (or intraoperative positioning devices) to improve the accuracy of component placement. We all recognize that a properly placed glenoid component will have longer-term survival than a malpositioned component. The second approach is to have non-standard glenoid components available to address the deformity. These can be either custom-made implants specific for the patient being treated or augmented “off the shelf” implants that address the common deformities encountered.
I have found that using non-custom or “off the shelf” augmented glenoid components have addressed many of the bone-loss issues I have encountered.
The authors actually combine both approaches – they use a custom implant with a specimen-specific guide. This could be perceived as the “best of both” but in actuality it is quite impractical from a cost perspective. The incremental cost of a custom implant combined with a CT-generated, patient-specific guide would add significant incremental cost. In 2016, regardless of where the surgery is being performed in the world, it is a surgeon’s responsibility to consider cost, especially in the context of cost vs. potential benefit. In addition, the FDA has been very strict on the use of custom implant components, which leaves us surgeons limited options for this approach.
I have found that using non-custom or “off the shelf” augmented glenoid components have addressed many of the bone-loss issues I have encountered. We are currently in the process of reporting our two-year results with these implants, which have been quite successful. Of course, the long term survival data (i.e., > 10 years) is most important to assess the true benefits.
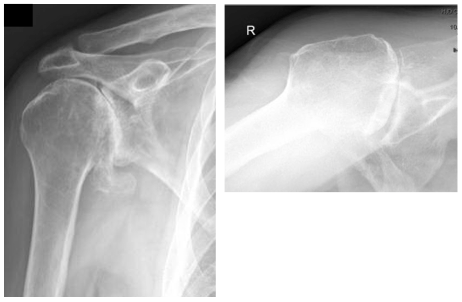
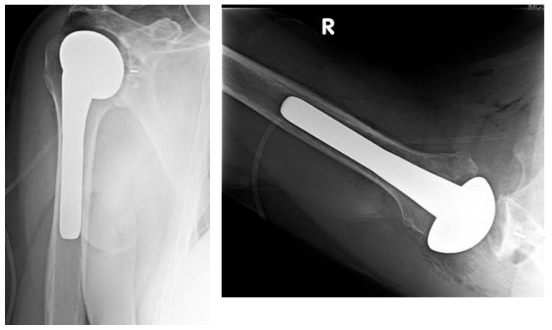
An example of this approach is shown in this case of a 62 year old male who underwent anatomic total shoulder replacement (TSR) using a 16 degree augmented glenoid component to correct posterior glenoid wear.

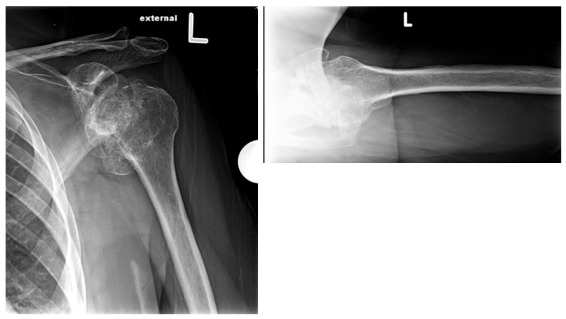
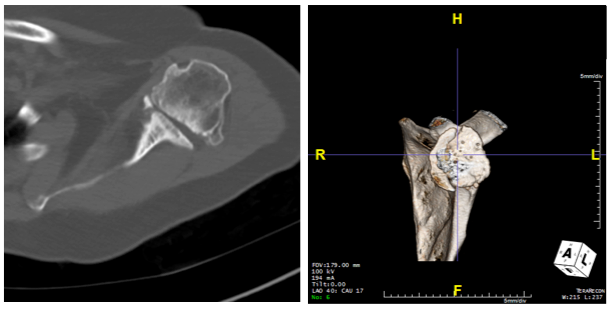
A second case shows an 8 degree posterior augmented glenoid baseplate in a 76 year old female who underwent reverse TSR for rotator cuff arthropathy.
In each of these cases intraoperative positioning software would have facilitated component placement, which for us, will be the next step in our approach to the glenoid.

In summary, I congratulate the authors on the design and implementation of the study. It has provided useful information for consideration by surgeons performing shoulder arthroplasty. However, concerns about the cost and practicality of the approach are anticipated to be important limiting factors.
Joseph Zuckerman, MD, is professor and chairman, and surgeon-in-chief at NYU Hospital for Joint Diseases. He completed his internship and residency at University of Washington, and fellowships at Brigham and Women’s Hospital and Mayo Clinic. Dr. Zuckerman is an industry thought leader and has traveled around the world educating surgeons on shoulder replacement. He is past president of the AAOS and an Equinoxe design team member.